
Downloads
Policy Context
The Inflation Reduction Act (IRA) of 2022 (P.L. 117-169) allows Medicare to negotiate prices with manufacturers for certain high-cost, single-source prescription drugs that are covered under Medicare Part B and Part D. The goal is to save money for both the Medicare program and beneficiaries. For Part D drugs, these negotiated prices, known as Maximum Fair Prices (MFPs), must be made available for enrollees at the pharmacy counter and other dispensing outlets, including mail-order services. However, doing so is complex and the timeline tight, as MFPs for the first 10 negotiated drugs covered under Part D are slated to take effect on Jan. 1, 2026. While the Centers for Medicare & Medicaid Services (CMS) is working with stakeholders to implement this program, manufacturers and pharmacies have expressed concerns about the operational challenges associated with the approach being taken.
This issue brief describes how CMS proposes to pass the negotiated prices to beneficiaries—a process referred to as “MFP effectuation.” It reviews the policy and operational framework behind MFP effectuation, including the options that CMS considered, and how the Medicare Transaction Facilitator (MTF) approach will work. Additionally, it details the roles and responsibilities of each stakeholder and the challenges faced in the implementation process, including potentially significant market disruptions and economic impacts to drug manufacturers and pharmacies if these challenges are not adequately addressed. While some of the issues discussed are also relevant for MFPs under Part B, numerous additional considerations are specific to MFP effectuation under Part B (first slated to take effect in 2028), which are not discussed herein.
Key Takeaways
- Medicare’s new drug-price negotiation authority marks a fundamental operational shift, requiring CMS to establish systems that deliver negotiated savings directly to Medicare beneficiaries.
- The first MFPs for 10 Part D drugs take effect on Jan. 1, 2026. The existing pharmacy distribution and reimbursement systems will be used to make MFPs available to beneficiaries, necessitating some adjustments to existing processes.
- Manufacturers can sell the selected drugs to pharmacies and other dispensing entities at the MFP through prospective purchase (direct sales to pharmacies at MFP) or retrospective refund (reimbursing pharmacies that sell at MFP after purchasing at the pharmacy’s acquisition price for the drug).
- CMS contracted for the development of a MTF to process claims data and facilitate refund payments between manufacturers and pharmacies under the retrospective model.
- Manufacturers and pharmacies—especially small independent pharmacies—have raised concerns about the MTF approach. Manufacturers cite aggressive refund processing timelines for millions of claims, while small pharmacies worry about cash-flow issues straining already slim margins.
- Operational challenges remain, including integration with existing programs, as CMS nears the Jan. 1, 2026, implementation deadline.
Introduction
Starting in January 2026, Medicare beneficiaries should be able to access federally negotiated prices for certain prescription drugs from their neighborhood pharmacies for the first time through authority granted to the Health and Human Services Secretary under the IRA (P.L. 117-169). The law allows the Secretary to negotiate directly with drug manufacturers the prices of some drugs that are used in both Medicare Parts B and D.
This marks a historic shift from the private-sector negotiation model established when Part D was launched in 2006 under the Medicare Modernization Act of 2003 (P.L. 108-173). Through the Medicare Modernization Act, price negotiations were delegated to private plans and pharmacy benefit managers. The act explicitly prohibited direct government intervention in determining drug prices for outpatient drugs distributed through pharmacies and covered under Part D. Successfully passing through Medicare’s negotiated MFPs to beneficiaries at point of sale would represent a remarkable achievement for CMS, given the program’s aggressive implementation timeline.2 However, stakeholders still indicate that they have major policy and operational issues with the decisions being made, and remain concerned that the agency will not have done adequate testing of the MTF systems necessary to assure successful implementation by the deadline.
The concept of governments negotiating with drug manufacturers is not novel, even in the U.S. context: Drug manufacturers have long negotiated drug prices with government purchasers. For example, the Omnibus Budget Reconciliation Act of 1990 (P.L. 101-508) established a program that provides minimum drug manufacturer rebates on prescription drugs to state Medicaid programs. States can also negotiate supplemental rebates with drug manufacturers. Similarly, the Veterans Health Care Act of 1992 (P.L.102-585) provided minimum statutory manufacturer rebates and discounts for prescription drugs to the Department of Veterans Affairs and Department of Defense prescription drug programs and to certain federally funded hospitals and clinics under the 340B Drug Discount Program.3
However, for the IRA to allow direct secretarial negotiations with drug manufacturers was a fundamental shift in the relationship with the federal Medicare program. For the first time, drug companies in the United States would have to directly negotiate drug prices with Medicare, the largest public-sector payer of prescription drugs, and even relatively small changes in pricing that represent a large volume of sales can generate financial disruption to the market. The relationship between Medicare, manufacturers and beneficiaries is also complex: Part D still requires beneficiaries to pay some out-of-pocket costs, such as deductibles and coinsurance, depending on the benefit design (low-income subsidy Medicare beneficiaries have a lower prescription copay structure). Finally, the IRA set an aggressive timeline for implementation. CMS was required to publish the first set of 10 drugs covered under Part D that were selected for negotiation by Sept. 1, 2023, about a year after the law’s passage, and negotiations on these drugs’ prices were set to be finalized approximately one year later.4,5 The negotiated prices become available to Medicare beneficiaries in January 2026, just three and a half years after the law was enacted.
The newly formed Medicare Drug Rebate and Negotiation Group (MDRNG) within the Center for Medicare was charged with implementing the new drug negotiation law. A key issue was how to make these negotiated prices available to beneficiaries. If the government negotiates drug prices but Medicare beneficiaries obtain their Part D prescriptions from such varied outlets as retail pharmacies, hospital outpatient departments and clinics, how do these lower negotiated prices transfer to pharmacies and other dispensers so they can pass them through to the beneficiaries? A brief overview of how the prescription drug distribution chain currently works will illustrate the challenges faced by the agency and the stakeholders in making these MFPs available to beneficiaries.
Overview of the Prescription Drug Distribution Chain
In the prescription drug distribution chain, manufacturers sell drugs to pharmaceutical wholesalers, who in turn sell them to healthcare facilities (e.g., pharmacies, hospitals, clinics) that dispense or administer the drugs to patients. Manufacturers produce medications, while wholesalers manage bulk purchasing and distribution. Wholesalers streamline logistics and maintain supply, so facilities can quickly access needed drugs—benefiting patients who depend on timely prescriptions.
Under the Part D program, CMS contracts through private health insurance plans to provide drug benefits to Medicare beneficiaries and work with pharmacies to dispense medications to enrolled beneficiaries. Traditionally, manufacturers and pharmacies negotiate directly with these plans—although frequently plans have enlisted pharmacy benefit managers (PBMs) to perform these and other services. Manufacturers offer the plans rebates and other price concessions in exchange for favorable coverage of their drugs (e.g., formulary placement), improving the likelihood that the Medicare beneficiary will have access to their drug.
Two key public pricing benchmarks underpin this distribution system. The wholesale acquisition cost (WAC) represents the manufacturer’s list price for selling drugs to wholesalers, serving as the baseline before any discounts or rebates. The average wholesale price (AWP) is a published benchmark price that functions as a standardized reference point throughout the industry. Despite its name, AWP is not actually an average of wholesale transactions but rather a “list price” established by the manufacturers and collected by drug pricing compendia publishers. Often, AWP is calculated as WAC plus 20% for a drug. While actual transaction prices are typically below these benchmarks due to various discounts and negotiations, both WAC and AWP serve as crucial reference points for contracts and reimbursement calculations across the distribution chain.
Separately, pharmacies negotiate with Part D insurance plans for their payment, which usually has two components: 1) an amount to reimburse the pharmacy for its purchase of the drug from the wholesaler (calculated as a percentage of the AWP) and 2) a dispensing fee. For example, a plan may pay a pharmacy an amount equal to AWP minus 19% plus $1 to dispense a drug to a Medicare beneficiary. In the normal course of business, the pharmacy would dispense the prescription and receive its payment from the Part D plan, plus any payment from the beneficiary (i.e., their share of costs under their plan). However, under the IRA, Part D plans reimburse pharmacies in amounts no more than the negotiated MFP for a selected drug. The plan, however, may be reimbursing pharmacies at amounts lower than the pharmacy’s purchase price for the drug. (The reference to “no more than the MFP” allows the plan to impose direct and indirect remuneration (DIR) fees on pharmacies, which could reduce their reimbursement for the drug to lower than the MFP amount.)7
Consider a single-source brand-name medication with a WAC of $80. In this case, the drug’s AWP is $96 (AWP=WAC X 1.2). A pharmacy might purchase this medication from a wholesaler for $76.80 (WAC minus 4%).8 When a Part D beneficiary fills a prescription for this drug, the insurance plan reimburses the pharmacy using a formula of AWP minus 19% (or 81% of AWP) plus $1 dispensing fee, which would equal $77.76 plus $1, or $78.76 total. In this scenario, the pharmacy would make a gross margin of about $2 ($78.76 reimbursement minus $76.80 acquisition cost) before accounting for its operational costs. The beneficiary’s cost-sharing would be calculated based on the plan’s reimbursement amount, so if they have a 25% coinsurance, they would pay approximately $19.69, while the plan would pay the remaining $59.07 to the pharmacy.
How the Inflation Reduction Act Changes the Process
To effectuate the MFP, the pharmacy makes this price available to the beneficiary at the point of sale. The beneficiary’s out-of-pocket cost depends on their coverage phase. Beneficiaries pay either the MFP plus a dispensing fee (if in the deductible phase) or cost sharing based on the MFP plus the dispensing fee (if in the coverage phase). However, if the drug was purchased by the pharmacy at its usual acquisition cost from the manufacturer, that manufacturer needs to compensate the pharmacy for the difference between its acquisition cost and the MFP at which it dispensed the drug.
If possible, pharmacies may be able to purchase the drug directly from the manufacturer or wholesaler at the MFP (Prospective Purchase—MFP Option 1 below) to avoid waiting to be made whole until after the drug has been dispensed. Because pharmacies usually make bulk drug purchases on behalf of all the patients they serve (not just Medicare beneficiaries), under the existing drug pricing paradigm, the responsibility falls on the manufacturer to compensate the pharmacy for the difference between the pharmacy’s acquisition cost and the lower MFP for sales to Medicare beneficiaries. This is referred to as a Retrospective Refund (MFP Option 2 below).
To make pharmacies whole, and to avoid manufacturers having to calculate or know each pharmacy’s drug acquisition cost to determine the refund, CMS suggested using the drug’s WAC price as the basis of the standard default refund amount to the pharmacy. Thus, the standard refund from the manufacturer to the pharmacy would be based on the drug’s published WAC minus the MFP.
Example of Pharmacy Payment for Maximum Fair Price (MFP) Drugs
Using the same hypothetical example from earlier, a single-source brand-name medication with a WAC of $80, AWP of $96, pharmacy acquisition cost of $76.80 and traditional Part D reimbursement of $78.76 (81% AWP plus $1 dispensing fee)—we can illustrate how the IRA’s MFP requirements would change the payment structure. Assume that this drug has been selected for negotiation and that CMS and the manufacturer have negotiated an MFP of $50. The table below demonstrates how the two MFP implementation options would affect the pharmacy’s costs, revenues and overall reimbursement compared to the current Part D payment structure.
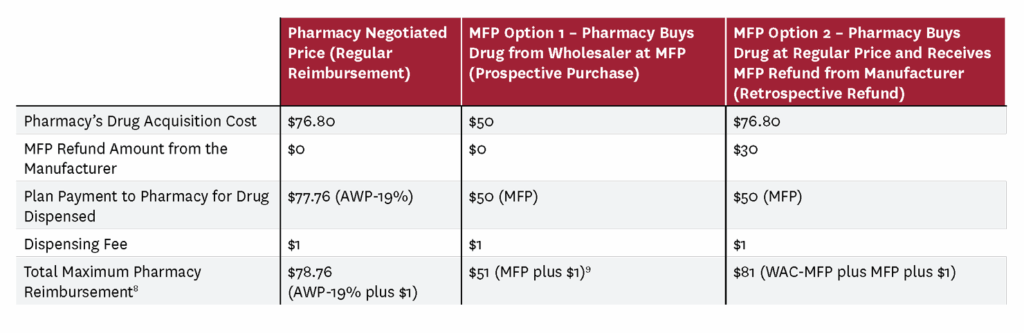
This example illustrates how the IRA changes pharmacy reimbursement dynamics. Under the prospective purchase option (Option 1), the pharmacy buys the drug directly at the MFP of $50 and receives the $1 dispensing fee as compensation. Under the retrospective refund approach (Option 2), the pharmacy maintains the same total reimbursement ($81) but through a different payment structure—$50 from the Part D plan plus a $30 manufacturer refund based on CMS’s standard WAC minus MFP calculation.
Background on the MFP Effectuation Process
The IRA provided the HHS Secretary with broad authority to carry out administrative duties in establishing the negotiation program,11 but it did not identify a specific role for the agency in the MFP effectuation or require that the agency hire an outside contractor to help manufacturers provide refunds to pharmacies for passing through MFP discounts to beneficiaries. Instead, the statute placed the burden of effectuation on the manufacturer of the selected drug.
However, manufacturers and pharmacies lack direct financial connectivity. As previously noted, there are several intermediaries (wholesalers, PBMs) between manufacturers and pharmacies who manage transactions with tens of thousands of pharmacy purchasers.
Given this lack of direct financial connectivity, stakeholders—particularly manufacturers and pharmacies—wanted CMS to undertake a significant role in MFP effectuation. The statute may have been silent on agency involvement, but stakeholders considered the participation of CMS to be essential in ensuring the negotiation program’s smooth administration. Having CMS take a role in effectuation, it was contended, would also help assure that Medicare beneficiaries could obtain the medications subject to an MFP at the pharmacy counter. Most stakeholders’ preferred approach was for the agency to implement MFP effectuation in the same manner that the Medicare Coverage Gap Discount Program (CGDP) had been implemented.
Medicare Coverage Gap Discount Program Approach to MFP Effectuation
Created by the Affordable Care Act of 2010 (P.L. 111-148), the Medicare CGDP provided eligible Part D beneficiaries with discounts at the point of sale for covered brand-name drugs.12 The manufacturer of these drugs must sign an agreement to offer these discounts in order for its drugs to be covered under Part D. The Medicare CGDP provided Medicare beneficiaries with discounts from drug manufacturers for Part D drugs during the coverage gap, thereby reducing beneficiary costs.13 In 2025, the program was replaced by the Medicare Discount Program (MDP), which, like its predecessor, requires drugs to be covered under an agreement between CMS and the manufacturer in order to be paid by Part D.
Under the MDP, the Part D plan advances manufacturer discounts to beneficiaries, reducing prices for the drug at the pharmacy point of sale. After dispensing a drug, the pharmacy bills the Part D plan for the full amount of the prescription, including any manufacturer discounts advanced by the pharmacy to the beneficiary. This sets up a seamless transaction: Pharmacies are paid as if all costs are covered by the plan, enabling beneficiaries to benefit from the manufacturer discounts immediately.
In order to ensure that plans have sufficient resources to pay pharmacies when drugs are dispensed under the discount program, CMS prefunds the money to plans on a monthly basis. The discounts provided by pharmacies to beneficiaries are then aggregated across Part D plans and invoiced to the contracted drug manufacturer on a quarterly basis. Manufacturers are required to pay the plans for the aggregated discounts within 38 days. Then the plans and CMS reconcile any outstanding balances annually.14 The Medicare CGDP statute gave specific authority to CMS to secure a third-party administrator contractor (TPA) to help operate the program and facilitate the payment process between manufacturers and plans. Though the statute did not give CMS specific authority to use a TPA for the MDP, CMS opted to continue using the same infrastructure for MDP as it had for CGDP. Neither the CGDP nor MDP statutes require prefunding plans for amounts due from manufacturers.
Pharmacies and manufacturers urged CMS to administer the MFP negotiation program in a similar manner to the CGDP. That is, Part D plans would pass through the MFP discounts to beneficiaries through pharmacies. Prefunded by federal monies, plans would pay pharmacies their full reimbursement for the selected drugs. Then the plans and manufacturers would “true up” the discounts on a periodic basis. However, the IRA did not give the agency the statutory authority to facilitate transactions through a CGDP approach.
Evolution of the Medicare Transaction Facilitator (MTF) Process
In its initial 2023 guidance, CMS proposed using a wholesaler-based chargeback system to make pharmacies and other dispensers whole.15 Under this approach, wholesalers would sell drugs to pharmacies at the reduced MFP (e.g., $50 instead of $76.80) and then bill manufacturers for the difference. Pharmacies could only dispense these discounted drugs to Medicare beneficiaries.
Rather than building a system totally around chargebacks,16 CMS chose to develop a MTF, a centralized system to handle claims data and payments for the MFP program. CMS already uses similar transaction facilitator models in Part D to allow pharmacists to determine beneficiary eligibility in real time.17 CMS awarded contracts for two components of the new system: an MTF Data Module (MTF-DM) and MTF Payment Module (MTF-PM).18
In this MTF system, claims data for selected drugs sent by pharmacies to Part D plans for payment would be routed to manufacturers through the data module. Manufacturers would then use this claims data to calculate their refunds to the pharmacies via the payment module. Currently, Part D plans submit claims data, called prescription drug event (PDE),19 to the CMS-operated Drug Data Processing System (DDPS).20 Under the MTF, relevant PDE data for a selected drug will be sent from the DDPS to the data module.21 These data will help manufacturers pay the refunds to the pharmacies for selected drugs—that is, the difference between the pharmacy’s cost of the selected drug and the MFP amount paid by the plan. In its 2025 guidance, CMS provided a graphic showing how the data flow works to effectuate the MFP for Part D drugs.22
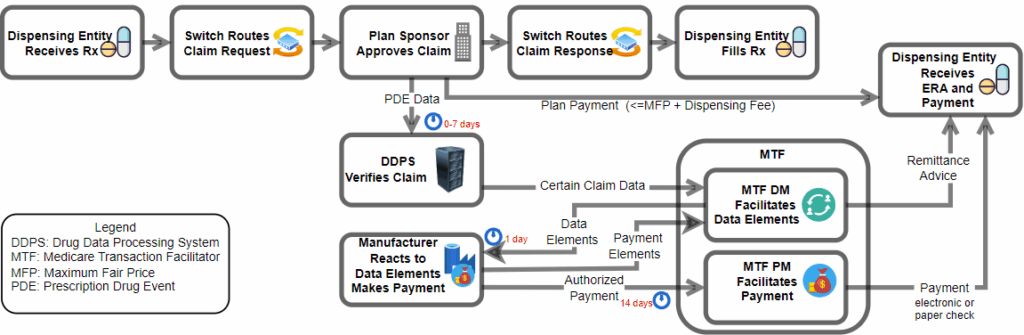
In summary, the MTF will operate in the following manner to effectuate the MFP:
- Manufacturer and pharmacy participation. Manufacturers must participate in the data module (and sign participation agreements, which include requirements relating to data security and privacy) to receive the Part D plan data to process claims for selected drugs. Manufacturer participation in the payment module is optional, but manufacturers not taking part must develop their own mechanisms for issuing MFP refunds to pharmacies. Pharmacies started enrolling in the data module in June 2025. When they enroll, pharmacies must sign agreements to garner MFP manufacturer refunds.23
- Pharmacies submit claims to Part D drug plans upon filling the prescription. The Part D plans receive the claim from the pharmacy, verify beneficiary eligibility and drug formulary coverage status, then authorize payment. Payment for selected drugs must not exceed the MFP amount plus the dispensing fee. Per existing Part D regulations, payment for the plan’s part of the selected Part D drug claim is to be made to the pharmacy within 14 days, and the pharmacy collects any beneficiary cost sharing at the point of sale.24 The payment timeframe will be longer for the portion of the refund coming from the manufacturer for the selected drug.
- Plan sponsors send prescription drug event (PDE) data to the Drug Data Processing System (DDPS). Part D plans have seven days after receiving the claim to send PDE data to DDPS.25 (This timeline was previously 30 days to send PDE data to DDPS, and that remains the timeline for non-selected drugs.) The seven-day deadline aims to accelerate the processing of MFP refunds to pharmacies. The DDPS conducts a second beneficiary eligibility check and other validation procedures to assure manufacturers that the beneficiary is eligible and the claim valid. This second data validation check in DDPS may reduce manufacturer anxiety regarding whether they are receiving valid claims. If edits to PDE data are needed, the system sends the claims back to Part D plans for correction.
- The DDPS forwards PDE data to the data module (MTF-DM), which then sends the claims to manufacturers. Upon receiving an MFP claim, the manufacturer has 14 days to determine how to handle it. Possible actions by the manufacturer include: paying the claimed MFP refund to the pharmacy; confirming that the drug was prospectively purchased by the pharmacy at the MFP and that no refund is due; determining that the drug was purchased under the federal 340B program, and not paying any refund if the price is lower than the MFP26; or concluding that insufficient information exists to pay the claim. Sometimes, Part D prescriptions are filled with drugs purchased under the 340B drug discount program. The IRA specifically indicates that the manufacturer is not required to provide an MFP on a drug when it is subject to a discount under the 340B program and the 340B price is lower than the MFP. This is a process known as “deduplication.” When the manufacturer receives claims from the MTF-DM, however, the 340B status of the claim will likely not be known because most 340B determinations are made after the claim has been filled and dispensed by the pharmacy. Therefore, it is up to the manufacturer to make that determination and then return that information to the data module so that no MFP refund would be authorized on that claim.
- Pharmacies receive payment and a reconciliation statement for claims from manufacturers. The MTF-DM then authorizes the payment module to pay the pharmacies from the manufacturer’s bank account for selected drug claims for which MFP refunds are due. Pharmacies receive an electronic remittance form27 from the data module detailing how each selected drug claim was disposed of by the manufacturer.
By Sept. 1, 2025, manufacturers had to submit plans to CMS explaining how they will work with the data and payment modules in MFP effectuation. The manufacturer details in these plans must include: whether they will participate in the MTF-PM (since taking part is optional); whether they will use WAC as the standard default refund amount for Part D refunds; and how they will avoid duplicate payments for drugs already receiving a 340B discount.
Manufacturer Concerns With the MTF Approach
As noted, the MTF-based method of effectuating the MFP under Part D was not the first choice of the manufacturer and pharmacy communities. In their public comments to the agency, both groups overwhelmingly preferred the Medicare CGDP model described above. Manufacturers voiced concerns with several challenges they face in implementing the MTF approach.
First, manufacturers indicated they had to build the internal infrastructure and processes to receive millions of Part D claims files from the data module on an ongoing basis and determine whether the claims are eligible for an MFP pharmacy refund. This determination must be done on an aggressive timeline—only 14 days—after manufacturers receive the claims from the data module.
Second, manufacturers must identify which claims involve 340B drugs to avoid double discounts (they shouldn’t pay MFP on drugs that already receive 340B discounts). At least 10% of all Part D claims are filled with 340B purchased drugs.28 Since manufacturers only have 14 days to decide whether to pay refunds, they must rely on other information like wholesale charge data to determine which claims might involve 340B drugs. If manufacturers determine that more claims were subject to 340B discounts than actually were, they may be vulnerable to potential audits of their obligations to provide 340B ceiling prices to 340B eligible entities—as well as possible penalties. Yet new proposed regulations from CMS and Health Resources and Services Administration (HRSA) may mitigate some of these concerns, as noted in the last section of this paper.
Third, manufacturers may face significant civil monetary penalties. These penalties would be imposed if CMS determines that manufacturers are not paying refunds to pharmacies within 14 days of receiving the claim from the data module, or if they are charging a price that is higher than the MFP. If manufacturers fail to make the MFP available, they will be penalized 10 times the difference between what they actually charged and the negotiated MFP. When assessing any penalties, CMS will give manufacturers an opportunity to justify the price that they made available and consider other such situations that might have led to the failure of the manufacturer to make the MFP available, such as technical issues relating to the operation of the MTF.
Fourth, manufacturers are also concerned that some pharmacies will claim that they have higher costs for drug acquisition than WAC—the suggested standard refund amount—and will seek refunds from manufacturers beyond the WAC-MFP amount. For example, CMS has proposed that when determining whether manufacturers have effectuated the MFP, they will assess whether manufacturers have paid the “commercially reasonable” costs that the pharmacy is likely to encounter in the distribution chain. This may require manufacturers to collect additional data from pharmacies to justify providing them with a refund greater than WAC minus MFP for the selected drug, such as pharmacy purchasing invoices.
Finally, manufacturers will have to decide how they can help pharmacies resolve the cash-flow issues that result from the longer payment cycle of MFP refunds. While manufacturers have expressed sympathy with the plight of the pharmacies, they are concerned that they will not be able to accurately assess whether pharmacies that self identify are truly having cash-flow issues and, if they are, what they can do to assist them. More details about this issue are included below.
Pharmacy Concerns With the MTF Approach
Pharmacies are a key component in making the MFP program work, given that they are the interface between the Part D plans and Medicare beneficiaries. However, pharmacies remain concerned that they are unfairly being put in the middle of the MFP refund-implementation process of the drug-negotiation program, and that it will result in significant economic hardship for them, especially as the number of drugs subject to negotiation increases over time.
First, pharmacies worry that Part D plans will continue to offer extremely aggressive reimbursement rates for Part D drugs, including the selected drugs with an MFP starting in January 2026. Because of the potential revenue impact from the refund payment lag, pharmacies asked CMS to require Part D plans to pay no less than the MFP (rather than no more than the MFP) for these selected drugs. Instead, CMS said it would monitor how Part D plans were reimbursing pharmacies for selected drugs and consider taking additional action if necessary to ensure beneficiary access.
Second, the MFP refund payment cycle timing may cause cash-flow problems for pharmacies. Pharmacies will have to wait at least 21 days to receive the MFP refund from manufacturers. (As noted previously, after a pharmacy submits a claim to the Part D sponsors, the plan has up to seven days to submit claims to the DDPS. The DDPS will likely take a day to process claims and send the file to the data module. Then manufacturers have 14 days to pay the refund.) This longer timeframe exceeds the current 14-day pharmacy prompt-payment requirement for traditional Part D claims.
Many pharmacies, especially small independent outlets, contend that they are already experiencing cash-flow issues caused by low reimbursements from Part D plans and other commercial payers. The National Community Pharmacists Association (NCPA) has sponsored several studies documenting the financial impact of the Medicare negotiation program on its membership. One such study found that a majority of NCPA members would not stock the first 10 Part D selected drugs, fearing they would have to dispense them at a financial loss that threatens their viability.29
As noted earlier, CMS created a process for pharmacies to self identify as having potential cash-flow issues related to the MFP process to address this concern. When they enroll in the data module, pharmacies can self identify as expecting cash-flow concerns when the program starts in January 2026. Manufacturers are required to include strategies to mitigate the impact of these pharmacy cash-flow issues in the plans they submit. But manufacturers have said that there is no statutory basis for this cash-flow mitigation approach and have raised significant operational and implementation concerns.
For example, it has been suggested that manufacturers accelerate the reimbursements to these pharmacies, rather than waiting 14 days to pay them. However, if this accelerated process reduces accuracy, manufacturers would have to reverse some of the payments made if the claims were not eligible for a refund because they were prospectively purchased at the MFP or a 340B claim. Manufacturers could also sell the selected drugs to pharmacies at the MFP price so that pharmacies wouldn’t have to wait for refunds. But this raises concerns that prospective sales of MFP drugs could lead to diversion to non-Medicare beneficiaries.
Another option proposed would be for manufacturers to prefund accounts based on the pharmacy’s utilization patterns for the selected drug. However, manufacturers worry that prefunding could violate federal anti-kickback statutes. That is, by prefunding an account for selected drugs that may be dispensed by a pharmacy, a manufacturer would be providing something of value to that pharmacy (e.g. advanced reimbursement) that may influence the purchase or utilization of drug by the pharmacy.30 Manufacturers would also need to ensure that any payment system works with their internal accounting processes and meets financial legal requirements.
The CMS final guidance for the Initial Price Applicability Year (IPAY) 2028 makes clear it believes that these pharmacy cash-flow challenges are temporary—happening just at the beginning of each year as dispensing entities adjust to the longer refund cycles for Part D drugs with MFPs. Pharmacies, however, believe that this is a more serious, long-term issue that threatens their viability. CMS has indicated that it will evaluate whether the pharmacy cash-flow self-identification process is a useful approach. The agency also emphasizes that it intends to prioritize expeditious pass-through of payment to pharmacies as it continues developing the payment module.
Future Considerations
Given the short implementation timeline, concerns by stakeholders, complex federal contracting and system design processes, and a change in administration, CMS faces a substantial challenge in getting the Part D drug effectuation component of the Medicare drug negotiation program up and running by January 2026.
As the agency continues to implement the program, it seems open to looking at ways of effectuating the MFP that might not be so complex for stakeholders. For example, the agency may be more open to looking at a prefunded model for drugs covered under Part D to mitigate pharmacy cash-flow concerns.
In addition, the agency has indicated that it is considering approaches to help manufacturers with the implementation challenges surrounding 340B and MFP claims. For example, in its final IPAY 2028 guidance, CMS says that it is “considering ways to incorporate asynchronous 340B data into MTF processes in the future.” CMS could collect claims information from third-party claims administrators of the 340B entities, enabling the data module to match Part D claims information with 340B data and remove those claims in which a 340B drug was priced lower than the MFP. Such a process, though, is likely years away, as CMS is still trying to find an approach to removing Part D claims filled with 340B drugs before they bill manufacturers for Part D inflation rebates.
In fact, in its proposed 2026 Physician Fee Schedule Rule,31 the agency did propose to establish a repository to which 340B covered entities could voluntarily submit claims data that would be used to identify Part D claims that were filled with 340B drugs such that these drugs would not be subject to Part D drug inflation rebates. This process may lay the groundwork for eventual use of the repository in the drug negotiation 340B-MFP deduplication process.
In addition, HRSA released a landmark notice32 on July 31, 2025, that establishes a one-year pilot program allowing manufacturers of the first 10 drugs subject to negotiation under Part D to effectuate the 340B ceiling price through a rebate model rather than an upfront discount to 340B covered entities. To date, HRSA has not permitted the use of a rebate to effectuate the 340B ceiling price. Manufacturers could only use an upfront discount. The goal of the pilot is to help manufacturers meet the requirement in the IRA statute that they not pay an MFP rebate on a drug that was already subject to a 340B ceiling price.
Under the model, manufacturers would change how they provide 340B discounts from the current upfront pricing system to a rebate system. Instead of selling drugs to covered entities at discounted ceiling prices, covered entities would purchase drugs at full wholesale price (WAC) and then receive rebates from the manufacturer. Covered entities seeking a refund would have to provide data to manufacturers, and manufacturers would have 10 days to pay the refund. In theory, this approach would reduce the chances for a duplicate discount being paid by the manufacturer, though covered entities argue that it increases their upfront purchasing costs. If successful, HRSA could make this program permanent and, as a result, reduce duplicate discounts in both Medicare and Medicaid.
For the new drug negotiation program to be successful, Medicare beneficiaries and the federal government will have to realize the savings from lower drug prices being negotiated by the agency. The MTF process will be an important part of the process of attempting to reach these goals. However, significant policy, legal and operational issues continue to challenge stakeholders.
Footnotes
- Coster served as a senior technical advisor to the Medicare Drug Rebate and Negotiation Group (MDRNG) in the Center for Medicare from August 2022 through February 2025 and director of the Division of Pharmacy for the Center for Medicaid and CHIP Services from August 2014 through August 2022, both within the Centers for Medicare & Medicaid Services (CMS). Disclosures reported by Coster are available here.
- The Inflation Reduction Act was enacted on Aug. 22, 2022, and the law required pass-through of MFPs for the first 10 drugs covered under Part D by Jan. 1, 2026.
- See Section 340B of the Public Health Service Act. The 340B Drug Discount Program allows certain federally funded clinics (e.g., community health centers, family planning clinics, Ryan White AIDS programs) and certain hospitals (e.g. Disproportionate Share Hospitals, rural hospitals, critical access hospitals) to purchase drugs from manufacturers at significantly discounted prices, known as a “ceiling price.” This price is based on a formula in the statute that essentially provides the equivalent of the manufacturer’s Medicaid rebate for the drug in the form of a discount to these entities. Drugs purchased at the 340B price by these entities are sometimes used to fill prescriptions for drugs dispensed to beneficiaries under Medicare Part D or administered under Part B.
- The list of first 10 drugs covered under Part D subject to negotiation was published on Aug. 29, 2023. www.cms.gov/files/document/fact-sheet-negotiation-process-flow.pdf.
- President Biden released the negotiated prices for the first 10 Medicare Part D drugs on Aug. 15, 2024, shortly before the 2024 national elections: https://bidenwhitehouse.archives.gov/briefing-room/statements-releases/2024/08/15/fact-sheet-biden-harris-administration-announces-new-lower-prices-for-first-ten-drugs-selected-for-medicare-price-negotiation-to-lower-costs-for-millions-of-americans/.
- See Section 1860D-2(d)(1)(D), which specifies that the negotiated price paid by the plan to the pharmacy is no greater than the MFP for such drugs plus any dispensing fees for such drug.
- DIR fees are charges that pharmacies pay back to Part D plans or PBMs. These fees are used to adjust payments to pharmacies based on their performance on quality metrics and other factors. Initially, DIR fees were assessed retroactively, sometimes months after a prescription was filled, but a 2024 change requires them to be reflected in the negotiated price at the point of sale. See www.cms.gov/newsroom/fact-sheets/medicare-part-d-direct-and-indirect-remuneration-dir.
- The WAC minus 4 percent estimate is based on the NADAC equivalency chart, which can be found at https://www.medicaid.gov/medicaid/prescription-drugs/downloads/retail-price-survey/nadac-equiv-metrics.pdf
- The maximum amount that the pharmacy would receive, as the plan may include additional fees, reducing these payment amounts.
- The pharmacy would not receive the $30 refund from the manufacturer, WAC-MFP, since the pharmacy purchased the drug at MFP.
- See Section 1191(a)(4) and Section 1196 of the IRA.
- These drugs are referred to as “applicable drugs” (defined at 42 CFR § 423.100 as a drug approved under a New Drug Application or a biological approved under a Biologics License Application).
- https://tpadministrator.com/internet/tpaw4.nsf/DID/Z0UWUE2UII.
- www.ecfr.gov/current/title-42/chapter-IV/subchapter-B/part-423/subpart-W.
- www.cms.gov/files/document/medicare-drug-price-negotiation-program-initial-guidance.pdf, see p. 65.
- CMS allows manufacturers to document the methods that they use to effectuate the MFP to pharmacies and other dispensers, which include chargebacks, ACH transactions, paper checks or e-vouchers.
- https://medifacd.mckesson.com.
- Data Computer Corporation of America was awarded the contract for development and administration of the MTF-DM, while National Government Services was awarded the contract to administer the MTF-PM.
- https://resdac.org/cms-data/files/pde.
- www.csscoperations.com/internet/csscw3.nsf/DID/MK00H9NFF6.
- Table 2 of the final Initial Price Applicability Year (IPAY) 2028 guidance includes the entire list of the data elements that manufacturers will receive for selected drug claims from the MTF. https://www.cms.gov/priorities/medicare-prescription-drug-affordability/overview/medicare-drug-price-negotiation-program/guidance-policy-documents.
- Another method that could have been used involved sending the claims to the MTF-DM through prescription “switches,” which route claims from the pharmacies to the relevant Part D plan/PBM. However, this would omit the second beneficiary validation check performed on the claim by the DDPS system. The second validation check gives manufacturers some assurance of the validity of the claim so they can pay the MFP refund to the pharmacy, if applicable, within the 14-day window.
- www.cms.gov/priorities/medicare-prescription-drug-affordability/overview/medicare-drug-price-negotiation-program/pharmacy-and-dispensing-entity-resources.
- See 42 CFR 423.520. “(1) Effective contract year 2010, the contract between the Part D sponsor and CMS must provide that the Part D sponsor will issue, mail or otherwise transmit payment with respect to all clean claims, as defined in paragraph (b) of this section, submitted by network pharmacies (other than mail-order and long-term care pharmacies) within—(i) 14 days after the date on which the claim is received, as defined in paragraph (a)(2)(i) of this section, for an electronic claim; or (ii) 30 days after the date on which the claim is received, as defined in paragraph (a)(2)(ii) of this section, for any other claim.”
- https://public-inspection.federalregister.gov/2025-06008.pdf. See 42 CFR 423.325, “A Part D sponsor must submit initial PDE records for selected drugs (as described at section 1192(c) of the Act) within 7 calendar days from the date the Part D sponsor (or its contracted first tier, downstream, or related entity) receives the claim.”
- Under the negotiation program, the manufacturer only has to provide the price which is lower for a selected drug—that is, the MFP price or the 340B ceiling price. The ceiling price is essentially the value of the Medicaid drug rebate for the drug in the form of a discount to the 340B entity.
- https://www.1edisource.com/resources/edi-transactions-sets/edi-835.
- Trends in Proportion of Medicare Part D Claims Subject to 340B Discounts, 2013-2020 | Health Policy | JAMA Health Forum | JAMA Network Volume 4, Number 11, published online Nov. 17, 2023.
- https://ncpa.org/newsroom/news-releases/2025/01/27/ncpa-cms-third-independent-pharmacies-wont-carry-drugs-negotiated.
- The Anti-Kickback Statute is a broad law that prohibits the knowing and willful payment of any form of “remuneration” (which includes cash or anything of value) to induce or reward referrals or business generation involving items or services (like prescription drugs) payable by federal healthcare programs such as Medicare and Medicaid. 42 U.S.C. § 1320a-7b(b).
- See Federal Register, Vol 90, No 134, July 16, 2025, p. 32352.
- https://www.federalregister.gov/documents/2025/08/01/2025-14619/340b-program-notice-application-process-for-the-340b-rebate-model-pilot-program.



